NHS activity and capacity during the coronavirus (COVID-19) pandemic: 29 April 2021
Data on coronavirus and NHS activity and capacity up to 27 April 2021.
In this page
In response to the coronavirus (COVID-19) pandemic, daily information on health care has been produced to support transparency and understanding of the NHS activity and capacity. The release includes figures on invasive ventilated beds by use, admissions and hospitalisations of COVID-19 related patients, and attendances to Accident and Emergency (A&E) departments.
Main points
- The number of new daily admissions with suspected or confirmed COVID-19 fluctuates, taking that into account, the 7 day rolling average has generally decreased since early January 2021 but has plateaued since early April 2021. The number of new daily admissions are currently at the lowest levels since reporting began on 1 April 2020.
- In the last 7 days, an average of 15 people a day were admitted to hospital as confirmed or suspected with COVID-19. This compares to an average of 18 for the week to 20 April 2021.
- The total number of beds occupied with COVID-19 related patients (confirmed, suspected and recovering) increased from the end of September 2020 and reached its highest level on 12 January 2021, at 2,879 patients. Since then, despite fluctuations, the number of beds occupied with COVID-19 related patients has decreased.
- As at 27 April 2021, 262 beds were occupied with COVID-19 related patients (confirmed, suspected and recovering), representing 3% of all hospitalisations. This is a decrease from 287 on 20 April 2021 (4% of all hospitalisations) and now at similar levels to September 2020.
- As at 27 April 2021, there have been reductions in the number of beds occupied with suspected and recovering COVID-19. The number of beds occupied with confirmed patients remains unchanged from the week ending 20 April 2021. Therefore, reductions in suspected and recovering COVID-19 patients have contributed to the overall decrease in the number of COVID-19 related patients.
- As at 27 April 2021, 4 invasive ventilated beds were occupied with COVID-19 related patients (confirmed and suspected), and are now at similar levels to September 2020. This compares to 8 on 20 April 2021 and to 164 at the peak in April 2020.
Accompanying tables for this release are available, including all the data shown below and also data concerning general and acute beds.
Statistics on 111 and NHS Direct calls, NHS staff absence and emergency ambulance calls are available on StatsWales as well as all other statistics in this release.
Additionally, information on beds, hospitalisations and admissions is published on weekdays at 12pm, on StatsWales containing data up to the previous day. After 12pm on Thursdays, the data shown in this release will not contain the most up to date published data. However, this weekly release provides additional commentary on trends in the data.
The data are taken from management information and are subject to change. They have not been subject to the same validation processes undertaken for official statistics releases. Where available, the official statistics should continue to be considered the authoritative source of data. Please see the Chief Statistician’s blog for more information on reporting management information, data quality and transparency.
Hospital activity and capacity
This section covers the number of admissions and hospitalisations of COVID-19 related patients and invasive ventilated beds occupied with COVID-19 related patients, to support transparency and provide an understanding of NHS activity and capacity during the COVID-19 pandemic.
Hospital coverage has changed over time, please see the quality and methodology section for more information.
Hospital admissions
Patients admitted to hospital as suspected or confirmed with COVID-19, from 1 April 2020 (MS Excel)
Notes
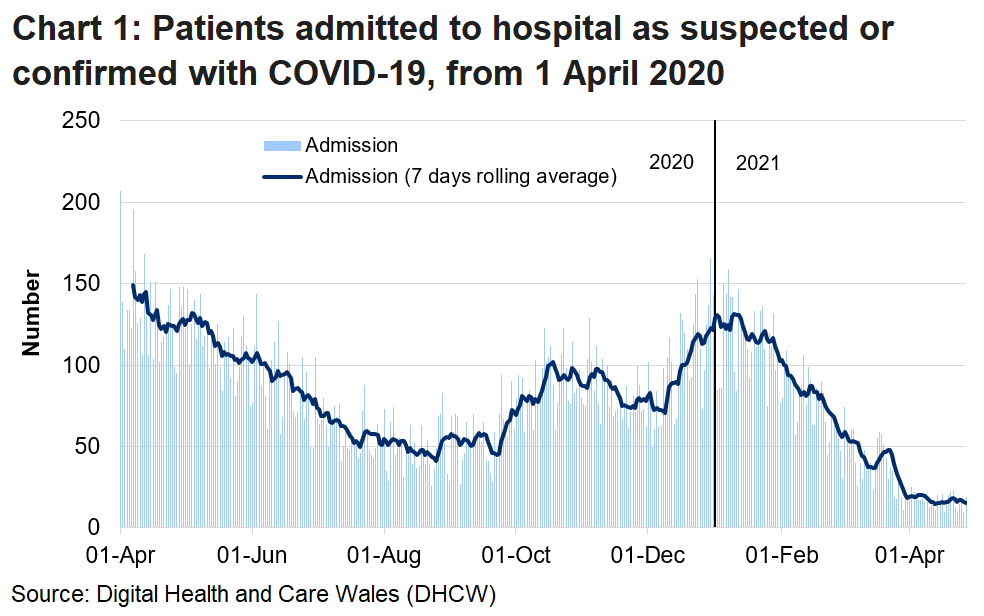
Admissions are the number of patients admitted to hospital between 9am on the update date and 9am the day before. COVID-19 related admissions include COVID-19 suspected or confirmed patients.
The health minister announced on 13 March 2020 that all non-urgent activity should stop to prepare for the pandemic.
From 3 July 2020, guidance was updated to only include emergency admissions in the COVID-19 related admissions figures.
From 29 June 2020, the guidance changed to explicitly ask health boards to exclude transfers between acute and community hospitals from admissions figures. Prior to this, some transfers may have been captured as new admissions.
From 29 June 2020, patients admitted for elective procedures were only included in COVID-19 related admissions if they received a positive COVID-19 test result on arrival at the hospital.
Following the re-introduction of elective procedures from June 2020, patients admitted for elective procedures suspected of having COVID-19 were initially captured in COVID-19 related admissions, even if they received a negative test later. This inflated the numbers of suspected cases in hospital at the time of reporting.
As at 27 April 2021
- The number of new daily admissions with suspected or confirmed COVID-19 fluctuates, taking that into account, the 7 day rolling average has generally decreased since early January 2021 but has plateaued since early April 2021. The number of new daily admissions are currently at the lowest levels since reporting began on 1 April 2020.
- In the last 7 days, an average of 15 people a day were admitted to hospital with confirmed or suspected COVID-19. This is 3 fewer admissions per day on average compared to 18 for the week to 20 April 2021.
Hospitalisations

Notes
Recovering patients was a category introduced on 26 May 2020 to capture patients who were COVID-19 positive in hospital and who showed no symptoms for 14+ days but remained in hospital on a COVID-19 treatment pathway, often for rehabilitation. There have been some differences in reporting by health boards in the time series which are outlined in more detail in the quality and methodology information section.
To ensure accurate and consistent reporting of Covid-19 recovering patients in the hospitalisations data, all health boards were reminded to follow the national guidance for SITREP reporting, and asked to ensure any necessary changes to their daily reporting were implemented by 12 April 2021. Contrary to the guidance, some health boards were counting long stay patients who had fully recovered from COVID-19 in the COVID-19 recovering category, rather than the non-COVID-19 category, which inflated the number of COVID-19 recovering patients. This change resulted in a step-change decrease in the number of recovering patients (a decrease of around 123 patients at the point of implementation). Whilst the impact was seen across most health boards, it mainly impacted the Swansea Bay University Health Board.
From 8 March 2021, Cardiff and Vale University health board have aligned their data more closely to the national guidance for SITREP reporting. This change has had a small impact on the hospitalisation figures resulting in a small increase in the number of confirmed COVID-19 patients and a small decrease in the number of recovering COVID-19 patients.
From 1 February 2021, guidance was reiterated to health boards that patients who were already in hospital and contracted COVID-19, but have now recovered and are back on their original setting, should be reported as non-COVID-19. This may affect a small number of patients who are in acute hospitals or mental health settings and may result in a decrease in recovering patients and an increase in non-COVID-19 patients.
From 18 January 2021, no patients occupying an invasive ventilated bed (critical care bed) should be counted as ‘recovering’ COVID-19 patients as they are still requiring a high level of care. Any patient previously reported as ‘recovering’ are now counted under ‘confirmed’. This resulted in an increase in the number of invasive ventilated beds occupied by ‘confirmed’ COVID-19 patients (an increase of around 14 patients at the point of implementation) and no invasive ventilated beds showing as occupied by ‘recovering’ patients. This change had no impact on the total number of COVID-19 related patients.
Please see the Chief Statistician’s blog for more information on reporting on recovering patients.
Main points
- The total number of beds occupied with COVID-19 related patients (confirmed, suspected and recovering) increased from the end of September 2020 and reached its highest level on 12 January 2021 (2,879 patients). Since then, despite some fluctuations, the total number has been generally falling.
- The numbers of confirmed COVID-19 patients and the number of recovering COVID-19 patients peaked at different times; with highest numbers of confirmed patients occurring early in January 2021 (1,643 on 4 January 2021) and highest numbers of recovering patients seen a few weeks later (1,192 on 31 January 2021).
As at 27 April 2021
- 262 beds were occupied with COVID-19 related patients (confirmed, suspected and recovering), representing 3% of all hospitalisations. This is a decrease from 287 (25 fewer occupied beds) on 20 April 2021 (4% of all hospitalisations) and now at similar levels to September 2020.
- There have been reductions in the number of beds occupied with suspected and recovering COVID-19. The number of beds occupied with confirmed patients remains unchanged from the week ending 20 April 2021. Therefore, reductions in suspected and recovering COVID-19 patients have contributed to the overall decrease in the number of COVID-19 related patients.
- 57 beds were occupied with confirmed COVID-19 patients, unchanged from 20 April 2021, and are at similar levels to mid-September 2020.
- 157 beds were occupied with recovering COVID-19 patients, a decrease from 171 (14 fewer occupied beds) on 20 April 2021, and now at similar levels to late October 2020.
- 48 beds were occupied with suspected COVID-19 patients, a decrease from 59 (11 fewer occupied beds) on 20 April 2021.
Invasive ventilated beds
Number of invasive ventilated beds by use, from 1 April 2020 (MS Excel)
Notes
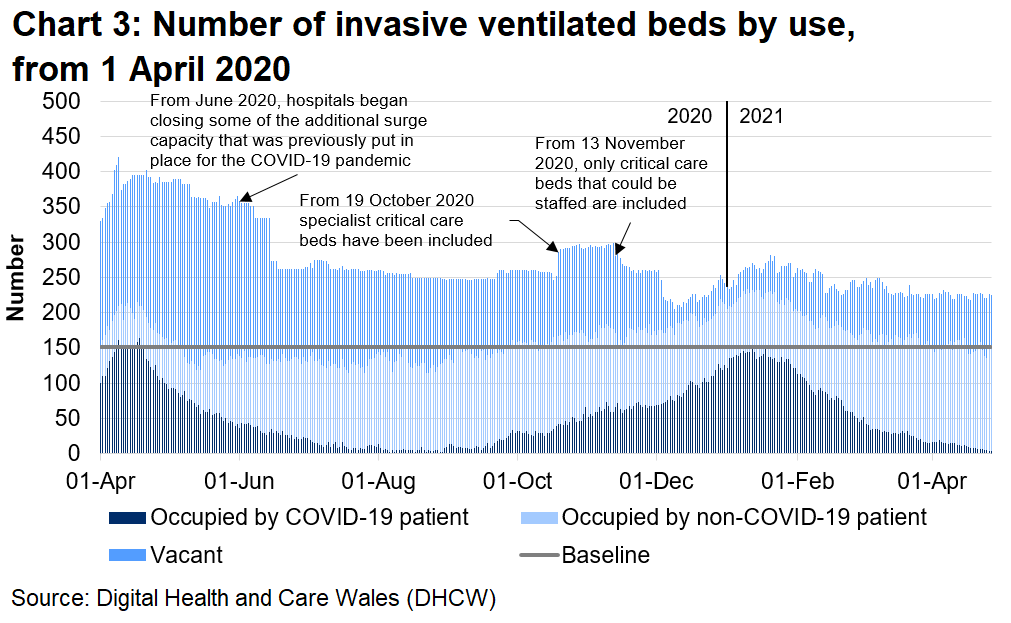
Baseline relates to the number of beds that were available prior to the COVID-19 pandemic. There are usually 152 critical care beds available. Invasive ventilated beds include beds in and outside a critical care setting, and include surge capacity. COVID-19 patients in this chart include suspected, confirmed, and recovering COVID-19 patients. Recovering patients are only included from 26 May 2020 to the 18 January 2021. Please see the note below and section quality and methodology information section for more detail.
From 18 January 2021, no patients occupying an invasive ventilated bed (critical care bed) should be counted as ‘recovering’ COVID-19 patients as they are still requiring a high level of care. Any patient previously reported as ‘recovering’ are now counted under ‘confirmed’. This resulted in an increase in the number of invasive ventilated beds occupied by ‘confirmed’ COVID-19 patients (an increase of around 14 patients at the point of implementation) and no invasive ventilated beds showing as occupied by ‘recovering’ patients. This change had no impact on the total number of COVID-19 related patients.
From 16 November 2020, data is included from the specialist and critical care Centre; Grange University Hospital in Aneurin Bevan University Health board. This increased the total number of beds available by around 450 beds.
From 13 November 2020, only critical care beds that could be staffed are included as available. Staffed beds are those that can be staffed at the time of the census. However, not all health boards implemented this change on that date. Following an update to guidance, more local health boards implemented this change from 4 December 2020. Please see the quality and methodology information section for more information.
From 19 October 2020 specialist critical care beds have been included in these figures. Please see the quality and methodology information section for more information.
From June 2020, hospitals began closing some of the additional surge capacity that was previously put in place for the COVID-19 pandemic.
As at 27 April 2021
- The number of occupied invasive ventilated beds generally increased from September 2020, reaching a high of 150 on 12 January 2021, but has decreased since to levels seen in September 2020.
- 4 invasive ventilated beds were occupied with COVID-19 related patients. This compares to 8 (4 fewer occupied beds) on 20 April 2021, and to 164 (160 fewer occupied beds) at the peak in April 2020.
- 151 invasive ventilated beds were occupied with non-COVID-19 related patients. This compares to 138 (13 more occupied beds) on 20 April 2021.
- There were 70 vacant invasive ventilated beds that could be staffed. This compares to 81 (11 fewer beds) on 20 April 2021.
Information on healthcare presented in the UK Government COVID-19 dashboard and in the Public Health Wales (PHW) dashboard differ from this publication. Please see the quality and methodology information section and the comparability with other publications section for more information.
A&E attendances
This section covers daily information on attendances to Accident and Emergency (A&E) departments in Wales, to further support transparency and provide an understanding of NHS activity and capacity during the COVID-19 pandemic.
The data are taken from management information and are subject to change. The latest data have not been subject to the same validation processes undertaken for official statistics releases. The official statistics should continue to be considered the authoritative source of data.
Please see the Chief Statistician’s blog for more information on reporting management information, data quality and transparency.
Number of daily A&E attendances to major and minor hospitals, from 1 January 2015 (MS Excel)
Notes
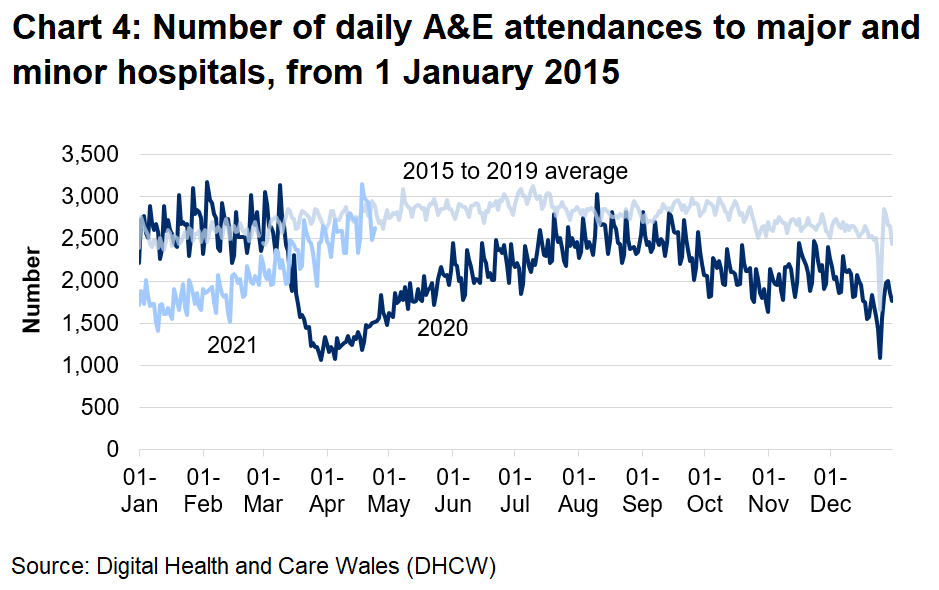
A&E attendances to major and minor hospitals, from all mode of transports across Wales. Some small minor A&E units are not able to submit daily data, therefore there is probably a small undercount in total attendance. The five-year average uses data from the years 2015 to 2019. For data on the 29 February, only data from the year 2016 and 2020 is included. There tends to be a lower number of attendances recorded on a Sunday compared to other days of the week and a higher recorded number of attendances in the summer compared to the winter.
Main points
- During March 2020, A&E attendances fell sharply to below half of the usual level. Attendances gradually increased from early April 2020, but generally remained below the 2015 to 2019 average.
- Since mid-January 2021, A&E attendances have been increasing, reaching similar levels to the 2015 to 2019 average.
Quality and methodology information
The data are taken from management information and are subject to change. They have not been subject to the same validation processes undertaken for official statistics releases. However, they are provided to support transparency and understanding of NHS activity at this time. The official statistics should continue to be considered the authoritative source of data.
Historic data are subject to revisions and therefore may differ slightly to previously published information.
Hospital activity and capacity
Following further validation, data prior to 1 April 2020 were decided to not be suitable for publication. Therefore, the time series begins on 1 April 2020.
Figures on hospital and activity include data from acute hospitals from 1 April 2020, field hospitals from 20 April 2020, community hospitals from 23 April 2020, mental health units from 10 July 2020, and exclude data from private hospitals.
To ensure accurate and consistent reporting of COVID-19 recovering patients in the hospitalisations data, all health boards were reminded to follow the national guidance for SITREP reporting, and asked to ensure any necessary changes to their daily reporting were implemented by 12 April 2021. Contrary to the guidance, some health boards were counting long stay patients who had fully recovered from COVID-19 in the COVID-19 recovering category, rather than the non-COVID-19 category, which inflated the number of COVID-19 recovering patients. This change resulted in a step-change decrease in the number of recovering patients (a decrease of around 123 patients at the point of implementation). Whilst the impact was seen across most health boards, it mainly impacted the Swansea Bay University Health Board.
From 8 March 2021, Cardiff and Vale University health board have aligned their data more closely to the national guidance for SITREP reporting. This change had a small impact on the hospitalisation figures resulting in a small increase in the number of confirmed COVID-19 patients and a small decrease in the number of recovering COVID-19 patients.
From 1 February 2021, guidance was reiterated to health boards that patients who were already in hospital and contracted COVID-19, but have now recovered and are back on their original setting, should be reported as non-COVID-19. This may affect a small number of patients who are in acute hospitals or mental health settings and may result in a decrease in recovering patients and an increase in non-COVID-19 patients.
From 18 January 2021, no patients occupying an invasive ventilated bed (critical care bed) should be counted as ‘recovering’ COVID-19 patients as they are still requiring a high level of care. Any patient previously reported as ‘recovering’ are now counted under ‘confirmed’. This resulted in an increase in the number of invasive ventilated beds occupied by ‘confirmed’ COVID-19 patients (an increase of around 14 patients at the point of implementation) and no invasive ventilated beds showing as occupied by ‘recovering’ patients. This change had no impact on the total number of COVID-19 related patients.
From 16 November 2020, data is included from the specialist and critical care Centre; Grange University Hospital in Aneurin Bevan University Health board. This increased the total number of beds available by around 450 beds.
From 13 November 2020, only critical care beds that could be staffed are included as available. Previously all critical care beds had been included regardless of whether they could be staffed. Staffed beds are those that can be staffed at the time of the census. General and acute beds only include beds that can be staffed. However, not all health boards implemented this change on that date. Following and update to guidance, more local health boards implemented this change from 4 December 2020.
From 19 October 2020, data for specialist critical care beds (such as those in Burns and Plastic in Morriston) and other specialist acute beds (such as maternity) across other acute sites have been included. These beds have been included in the data as they are part of the available bed stock, and may be used for COVID-19 patients in exceptional circumstances. The majority of these beds are not occupied with COVID-19 patients. Therefore the inclusion of these had very little impact on the number of beds occupied with COVID-19 patients but a larger impact on vacant beds and those occupied with non-COVID19 patients.
Data from mental health units were included retroactively from 10 July 2020 for the first time in the release on 20 August 2020. The inclusion of mental health beds had a small impact on beds occupied with COVID-19 patients’ figures but a large impact on all beds occupied with non-COVID19 patients and vacant beds, as the majority of mental health beds are not occupied by COVID-19 patients. Mental health units’ data are submitted each Friday, and the Friday position is used as proxy for the following week, unless there is a major change in circumstances.
On reporting recovering patients, Aneurin Bevan started reporting recovering patients from 7 June 2020, but these were captured in the confirmed COVID-19 category before. Cardiff and Vale classified recovering patients as non-COVID-19 patients between 1 May 2020 and 22 May 2020. Following the change in guidance, Cardiff and Vale re-categorised these patients as COVID-19 patients, capturing them in the confirmed COVID-19 category until the recovering category was introduced on 26 May 2020.
Comparability
Please see the UK Government COVID-19 dashboard for information on healthcare at a UK level. Note: the healthcare data presented in the UK dashboard differs from this publication. Data for Wales on the UK dashboard includes data for acute hospitals only which was initially provided to enable better comparability with other countries. Whereas this publication includes data from acute, community, field hospitals and mental health units to provide a more comprehensive view of the system in Wales. From 11 December 2020, data for England presented on the UK dashboard was updated to align with NHS England publications and as a result the full time series for this item was revised. Data for England on the UK dashboard now includes data from acute, community, field hospitals and mental health units. Due to this reporting change, we are reviewing the suitability of data currently provided for Wales. Estimates of the number of people who had coronavirus in England and Wales is also published by the Office for National Statistics in their Coronavirus (COVID-19) Infection Survey.
Please note that health care surveillance data presented in the Public Health Wales (PHW) dashboard differ from this publication. The PHW dashboard uses data systematically collected through ICNET, the hospital infection control data system used across Wales. It includes hospital in-patients with a laboratory confirmed result and does not count any patients who were admitted and discharged on the same day.
The Welsh Government publication uses data sourced from daily management information provided by health boards. Guidance was issued to local health boards for completion and submission of the data return. However, data collection methods may vary between health boards. It includes COVID-19 related patients as suspected, confirmed and recovering, as well as non-COVID-19 patients.
The narrower definition used by PHW will likely result in smaller numbers of reported COVID-related admissions compared to the Welsh Government publication, but provides a systematic way of carrying out surveillance of patients requiring hospital stays with confirmed COVID-19.
National Statistics status
These statistics are not National Statistics. However, as far as has been practicable, they have been collected and validated in accordance with the pillars and principles within the Code of Practice for Statistics. We continue to develop the data collection and quality assurance process to improve the data.
These statistics have been produced quickly in response to developing world events.
Well-being of Future Generations Act (WFG)
The Well-being of Future Generations Act 2015 is about improving the social, economic, environmental and cultural wellbeing of Wales. The Act puts in place seven wellbeing goals for Wales. These are for a more equal, prosperous, resilient, healthier and globally responsible Wales, with cohesive communities and a vibrant culture and thriving Welsh language. Under section (10)(1) of the Act, the Welsh Ministers must (a) publish indicators ('national indicators') that must be applied for the purpose of measuring progress towards the achievement of the wellbeing goals, and (b) lay a copy of the national indicators before Senedd Cymru. The 46 national indicators were laid in March 2016.
Information on the indicators, along with narratives for each of the well-being goals and associated technical information is available in the Well-being of Wales report.
Further information on the Well-being of Future Generations (Wales) Act 2015.
The statistics included in this release could also provide supporting narrative to the national indicators and be used by public services boards in relation to their local wellbeing assessments and local wellbeing plans.
Next update
The next release will be at 9.30am Thursday 6 May 2021.
Contact details
Statistician: Alex Fitzpatrick
Telephone: 0300 025 9016
Email: kas.covid19@gov.wales
Media: 0300 025 8099
SFR 130/2021