Technical Advisory Group: COVID-19 population immunity estimates in Wales
Estimating COVID-19 population immunity in Wales through modelling.
This file may not be fully accessible.
In this page
Key points
Assuming immunity wanes after 2 years, 82% [64%, 85%] of people aged 16 and over in Wales were estimated to have had some immunity against COVID-19 infection at 24 July 2021.
Assuming immunity wanes after 2 years, 70% [56%, 72%] of the total population in Wales were estimated to have had some immunity against COVID-19 infection at 24 July 2021.
Immunity levels varied across age groups. Highest immunity was estimated in individuals aged 80 and over at 97% [70%, 97%] at 24 July 2021. Lowest immunity (excluding individuals aged under 16) was estimated in individuals aged 16 to 19 at 55% [53%, 61%] at 24 July 2021.
Immunity levels in the population have been significantly increased by the vaccine rollout. If no vaccines had been administered, it was estimated that 34% of people aged 16 and over in Wales (32% of the total population) would have had some immunity against COVID-19 infection at 24 July 2021.
It is estimated that over 80% (may be closer to 90%) of the Welsh population, spread evenly across Wales, must be immune to COVID-19 before population immunity effects could be observed.
Background
COVID-19 has existed for over 18 months and natural immunity has built up in the population following infections. On top of that, deployment of vaccines has further increased immunity to COVID-19 infection. It is estimated that over 80% (may be closer to 90%) of the Welsh population, spread evenly across Wales, must be immune to COVID-19 before population immunity effects could be observed.
Despite an average vaccine first dose uptake of 87% in those aged 16 and over in Wales (72% of the total population), it will be extremely difficult, if possible, to reach population immunity. Factors affecting the likelihood of achieving population immunity include: lower vaccine uptake in younger age groups, a significant proportion of those aged under 18 being ineligible for vaccines, a non-uniform distribution across Wales and across age groups, R0 of the dominant delta variant and other emerging variants, the proportion of individuals immune from natural infection, the possibility of waning immunity and the need for booster vaccines, the possibility of emerging variants with increased transmissibility or mortality risk or ability to escape immune responses, and evidence that vaccines are not 100% effective.
Methods
The term “COVID-19 immunity” can mean protection from COVID-19 infection, protection from severe illness, and/or prevention/reduction of transmission of COVID-19 to others. In this analysis, immunity refers to individuals who are no longer able to be infected with COVID-19 (until an individual’s immunity starts to wane over time). In this model, people who are ‘immune’ will no longer be infected with COVID-19 in the model, including asymptomatic cases.
The proportion of Wales’ population with some immunity to COVID-19 between early 2020 and 24 July 2021 was estimated. In this model, individuals were considered to build immunity 14 days after a COVID-19 infection or an effective COVID-19 vaccination. Individuals were modelled to remain immune for a certain number of days defined by the waning immunity assumption applied in the model. The three waning immunity scenarios modelled are reported in Table 1.
|
Scenario |
Time period after which immunity is assumed to wane |
|
1 - Default |
2 years |
|
2 |
10 months |
|
3 |
7 months |
In the default analysis, it was assumed that immunity from infection or effective vaccination waned after 2 years. Two scenario analyses were carried out to assess the impact of immunity waning more quickly; after 10 months and after 7 months. When an individual’s immunity waned, they were modelled to move from the “immune” population to the “susceptible” population. See Model assumptions for more information on waning assumptions.
Immunity levels have been estimated for the following age groups in Wales: total population, individuals aged 16 and over, individuals aged 16 to 19, 20 to 29, 30 to 39, 40 to 49, 50 to 59, 60 to 69, 70 to 79 and individuals aged 80 and over. Assumptions for waning immunity, vaccine efficacy and the time it takes to build immunity following a COVID-19 infection or vaccination were kept constant for all age groups.
In reality, waning immunity may be different for natural infections and for different types of vaccine, and different for different age groups. In this analysis, the same waning immunity assumption is applied across all age groups for infections and vaccinations as data is not yet available to separate these out.
The vaccine rollout began on 7 December 2020. Table 1 reports the vaccine efficacy assumptions used in the model.
|
Vaccine |
Efficacy against infection |
|
|
First dose |
Second dose |
|
|
Oxford-AstraZeneca |
34% |
64% |
|
Pfizer-BioNTech |
56% |
80% |
|
Moderna |
56% |
80% |
For the central immunity estimate, it was assumed that vaccine effectiveness was the first dose efficacy following a first dose and the second dose efficacy following a second dose, accounting for a 14-day time period between vaccine administrations and building of immunity. For the lower immunity estimate, it was assumed that vaccine effectiveness was the first dose efficacy following a first or a second vaccine dose. For the higher immunity estimate, it was assumed that vaccine effectiveness was the second dose efficacy following first or a second vaccine dose.
The following formula was used to calculate the number of people in Wales immune to COVID-19 infection on a given date:
|
Number immune to COVID-19 |
= |
Number immune following infection (84% of infections lead to immunity [footnote 2]) |
+ |
Number immune following effective vaccination (using vaccine efficacy data)
|
- |
Number immune from infection and vaccination (to prevent double-counting of immunity) |
|
Data source |
Description |
|---|---|
|
PHW vaccine data |
First and second doses by vaccine type, date of administration and age group of recipient |
|
PHW cases data |
PCR-confirmed positive coronavirus tests by date of result authorisation and age group of individual |
|
ONS population estimates: mid-2020 |
Used to estimate the population size of each age group in Wales |
|
Swansea University modelled cases |
Most Likely Scenario as at November 2020 used to estimate the true number of infections between January 2020 and December 2020 before widespread community testing was available |
|
ONS COVID-19 Infection Survey |
Modelled percentage of the adult population testing positive for antibodies to SARS-CoV-2 in Wales |
Model assumptions
Table 2 shows the vaccine efficacy assumptions used in the model to determine the number of individuals that became immune following a first or second vaccine dose.
Immunity was assumed to wane after a defined number of days had passed since immunity was first built. Table 1 shows the waning immunity scenarios modelled in this analysis. In the default scenario, immunity was assumed to wane after 2 years. This time period was based on time to waning immunity of other coronaviruses [footnote 3]. Since the COVID-19 pandemic started less than 2 years ago, no individuals were modelled to have had their immunity wane up to July 2021 in the default scenario. Studies have reported that antibodies are detectable for at least 6 months and probably 8 months or more [footnote 4]. The SIREN study reported that a previous history of SARS-CoV-2 infection was associated with an 84% lower risk of infection, with median protective effect observed 7 months following primary infection [footnote 5]. The Vivaldi study reported that natural immunity to COVID-19 substantially reduced the risk of reinfection for approximately 10 months following primary infection [footnote 6]. Therefore, scenarios were modelled assuming immunity waned after 7 months and 10 months.
In addition to the vaccine efficacy and waning immunity assumptions, Table 4 reports the assumptions applied to all age groups in the model, all waning immunity scenarios, with and without COVID-19 vaccines being deployed, for calculating the estimated immunity in the population of Wales.
|
Assumption |
Value |
|---|---|
|
Immunity estimates had COVID-19 vaccines not been deployed |
Swansea University Epidemiological models with a 0% vaccine efficacy were used to model immunity in the Welsh population had no vaccines been administered. |
|
Population size in Wales |
ONS mid-2020 population estimates [footnote 7] were used. It was assumed there had been no change in the population size of each age group. This is believed to be an under-estimate of the population. |
|
Pre 5 December 2020 proportion of infections |
Proportion of cases attributed to each age group was determined as the percentage of the population in that age group. |
|
Pre 5 December 2020 number of infections |
Number of infections estimated by Swansea University Epidemiological models from November 2020 [footnote 8] multiplied by the assumed proportion of infections in that age group. |
|
Post 4 December 2020 number of infections |
PHW ICNet cases data, excluding cases labelled as "Outside Wales" or “Unknown”, divided by the percentage of infections captured by a PCR test. |
|
Number of first and second vaccine doses administered in Wales |
PHW vaccines data, excluding cases labelled as "Outside Wales" or “Unknown”. |
|
Percentage of infections captured by a COVID-19 PCR test |
40%[footnote 9] |
|
Percentage of COVID-19 infections that lead to immunity |
84%[footnote 10] |
|
Percentage of vaccine doses that lead to immunity |
Vaccine efficacy assumptions in Table 2. |
|
Length of time for immunity to build following a positive PCR test result for COVID-19 infection |
14 days. |
|
Length of time for immunity to build following a vaccine dose |
14 days. |
|
Building immunity after a COVID-19 infection or effective vaccination |
An individual’s immunity is assumed to build from 0% to 100% immune on the date modelled to build immunity. |
|
Losing immunity from a COVID-19 infection or effective vaccination |
An individual’s immunity is assumed to wane from 100% to 0% immune on the date modelled to lose immunity. |
|
Length of time for immunity to wane |
Waning immunity scenarios in Table 1. |
|
Vaccine-derived and infection-derived immunity overlap assumption |
A percentage of those vaccinated will have already acquired immunity from a natural COVID-19 infection. The number of people moving from infection-derived immunity to vaccine-derived immunity is calculated as the number of people gaining immunity today from a vaccination, multiplied by the current immunity level from infections alone, multiplied by the percentage of people who have not already received at least one vaccine dose. This prevents double-counting of immunity levels in the population from natural infection and vaccination. |
Model limitations
The number of infections prior to vaccination rollout in December 2020 were estimated by apportioning the Swansea University Nov-2020 epidemiological Most Likely Scenario model by the proportion of actual confirmed COVID-cases by age band. This is a limitation because cases in certain age groups are more likely to be detected than in others (i.e. older adults are more likely to be symptomatic and get tested for COVID-19 than younger adults).
There is still a large amount of uncertainty in the effectiveness of COVID-19 vaccines. When new variants arise, it can take time to gather enough data to obtain accurate vaccine efficacy estimates. Therefore, vaccine effectiveness estimates are updated frequently as new evidence becomes available and as new variants of SARS-CoV-2 appear.
Immunity was assumed to increase from 0% to 100% after 14 days following either an effective vaccination or COVID-19 infection (in 84% of infections). Similarly, immunity was assumed to wane from 100% to 0% after a defined number of days since last infection or vaccination. In reality, immunity will build or taper over time.
Vaccine-derived immunity was assumed to wane after the same time period as immunity from natural infection. However, it is likely that vaccine-derived immunity will wane earlier as most vaccines target the spike protein whereas natural infection gives a broader repertoire of responses to fight the virus.
In this analysis, individuals were not followed day-by-day; individuals were modelled as a proportion of the population. Therefore, this model produced immunity estimates as an average for the population. In reality, immunity will vary between individuals – an individual may be less likely to be infected after exposure or vaccination, but it will depend on many factors, such as how many times they encounter an infectious individual, what kind of contact they have and what viral load the infectious individual has. Being exposed to the virus may boost immunity in individuals without them becoming infected. So an individual may have 80% immunity, but this may not be the same as 80% of a population having immunity.
Immunity compared with antibody positivity
Immunity is extremely difficult to measure directly, hence a direct comparison is not available. Antibody positivity offers an indication of immunity and it is useful to compare immunity estimates from this analysis to ONS antibody estimates. However, it’s not fully understood how having detectable antibodies affects the likelihood of being infected with COVID-19. There are other parts of the immune system (such as T cell response [footnote 11]) to consider which also offer protection. Therefore, it’s important to recognise that having antibodies to COVID-19 doesn’t necessary mean having immunity to it. Further reasons ONS’ antibody positivity is not directly comparable to this analysis’ immunity estimates include:
- ONS antibody estimates are based on study participants who have volunteered for the COVID-19 Infection Survey and the results are extrapolated. There is a risk of sample bias, non-response bias and uncertainty from extrapolating results from a relatively low number of observations to the whole Wales population.
- ONS antibody estimates are based on the community population aged 16 years and over, which excludes people in care homes or hospitals. Therefore, ONS’ antibody estimates may not be fully-representative of the entire population of Wales aged 16 and over. Immunity estimates are based on the whole Wales population aged 16 and over.
- After vaccination or COVID-19 infection, an individual may produce antibodies as part of the body’s immune response. Therefore, presence of antibodies is an indication, but not a guarantee, of immunity to COVID-19.
- ONS’ antibody positivity estimates use 2019 mid-year population estimates. The immunity estimates in this analysis used 2020 mid-year population estimates.
For all scenarios in this analysis, immunity estimates were lower than the most recent antibody estimates reported by ONS. This could be due to a number of reasons, such as under-estimating vaccine efficacies, inaccurate assumptions about the overlaps between those who have been both infected and vaccinated, or modelled data not representing the true picture. Additionally, there may be sample bias in the ONS COVID-19 Infection Survey could have led to overestimation of antibody positivity.
Results
Vaccination status
Figure 1: Vaccination uptake of first and second doses for individuals aged 16 and over in Wales
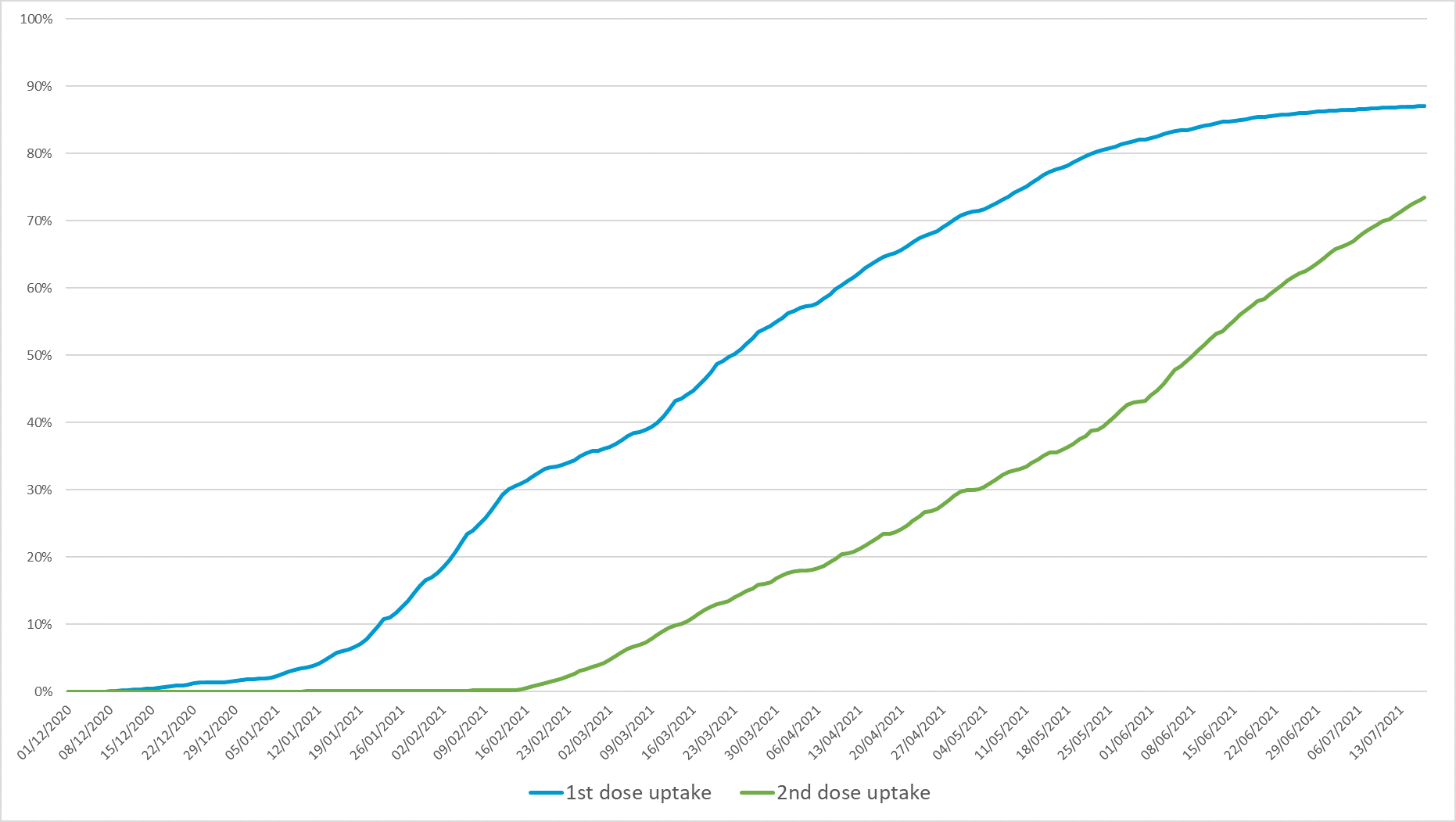
Figure 1 shows that administration of first COVID-19 vaccine doses for those aged 16 and over in Wales slowed shortly after vaccinations were opened to the final age group (aged 18 and over) in May 2021. At 24 July 2021, 87% of people aged 16 and over had received a first dose, but although this percentage was still slowly increasing, it had largely plateaued. At 24 July 2021, 76% had received a second dose and this percentage was still increasing at a steady rate.
Figure 2: Vaccination and antibody status of individuals aged 16 and over in Wales.
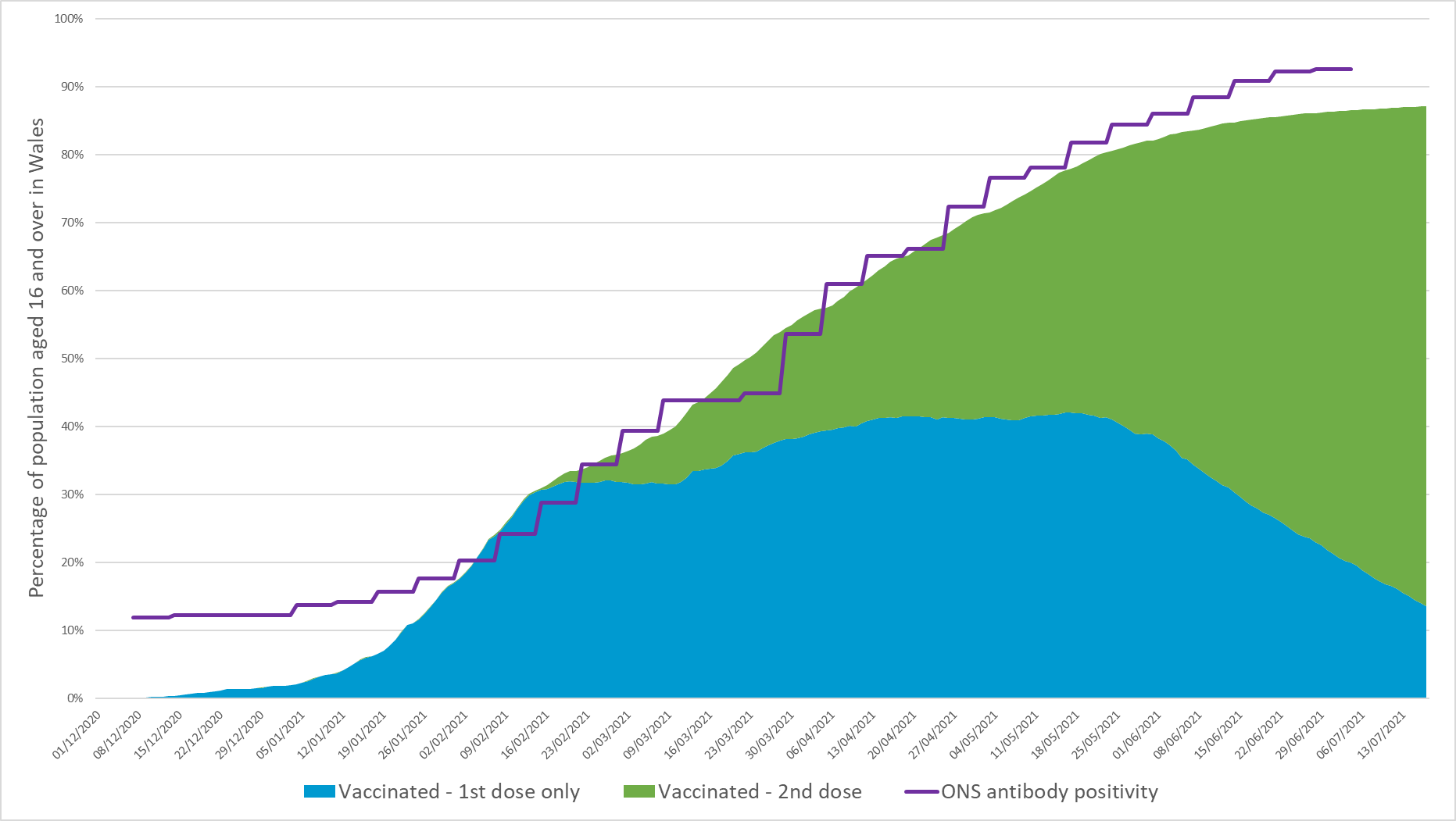
The slowing of first dose administration can be observed in Figure 2 by the blue wedge, which is tapering down as a higher percentage of individuals become fully vaccinated. As at 24 July 2021, 87% of people aged 16 and over had received at least one COVID-19 vaccine dose in Wales. 11% of people aged 16 and over had exactly one vaccine dose and 76% were fully vaccinated.
Figure 2 also shows ONS’ modelled percentage of the adult (aged 16 and over) population testing positive for antibodies to SARS-CoV-2 in Wales. Between 28 June and 4 July 2021, the ONS COVID-19 Infection Survey estimated that 92.6% of the community population aged 16 and over in Wales tested positive for COVID-19 antibodies.
Interestingly, ONS’ antibody positivity estimate increased at a similar rate to vaccination uptake between January 2021 and April 2021. However, after April 2021, although the vaccination uptake rate slowed, ONS’ antibody positivity estimate continued to increase at a steady rate.
Therefore, it is surprising that antibody positivity increased at a similar rate to vaccine uptake during spring 2021 when cases (and so building of antibodies from natural infection) were low. This illustrates the complexity of estimating immunity and highlights that antibody positivity is an indicator of immunity, but does not equal immunity.
Immunity estimates assuming immunity wanes after 2 years
Table 5 shows that 82% of individuals aged 16 and over in Wales and 70% of the total population in Wales were estimated to be immune to COVID-19 as at 24 July 2021. Without the introduction of COVID-19 vaccines, it was estimated that 34% of individuals aged 16 and over and 32% of the population would have been immune at 24 July 2021.
|
Age group |
Immunity [lower, upper] estimate |
Immunity estimate without vaccines |
|---|---|---|
|
16-19 |
55% [53%, 61%] |
38% |
|
20-29 |
78% [72%, 86%] |
46% |
|
30-39 |
86% [74%, 91%] |
43% |
|
40-49 |
87% [67%, 89%] |
36% |
|
50-59 |
89% [64%, 88%] |
31% |
|
60-69 |
82% [55%, 81%] |
21% |
|
70-79 |
86% [60%, 86%] |
17% |
|
80+ |
97% [70%, 97%] |
41% |
|
Total (all ages) |
70% [56%, 72%] |
32% |
|
Total (16+) |
82% [64%, 85%] |
34% |
Figure 3: immunity estimates and antibody status of individuals aged 16 and over in Wales, to 24 July 2021, assuming immunity wanes after 2 years.
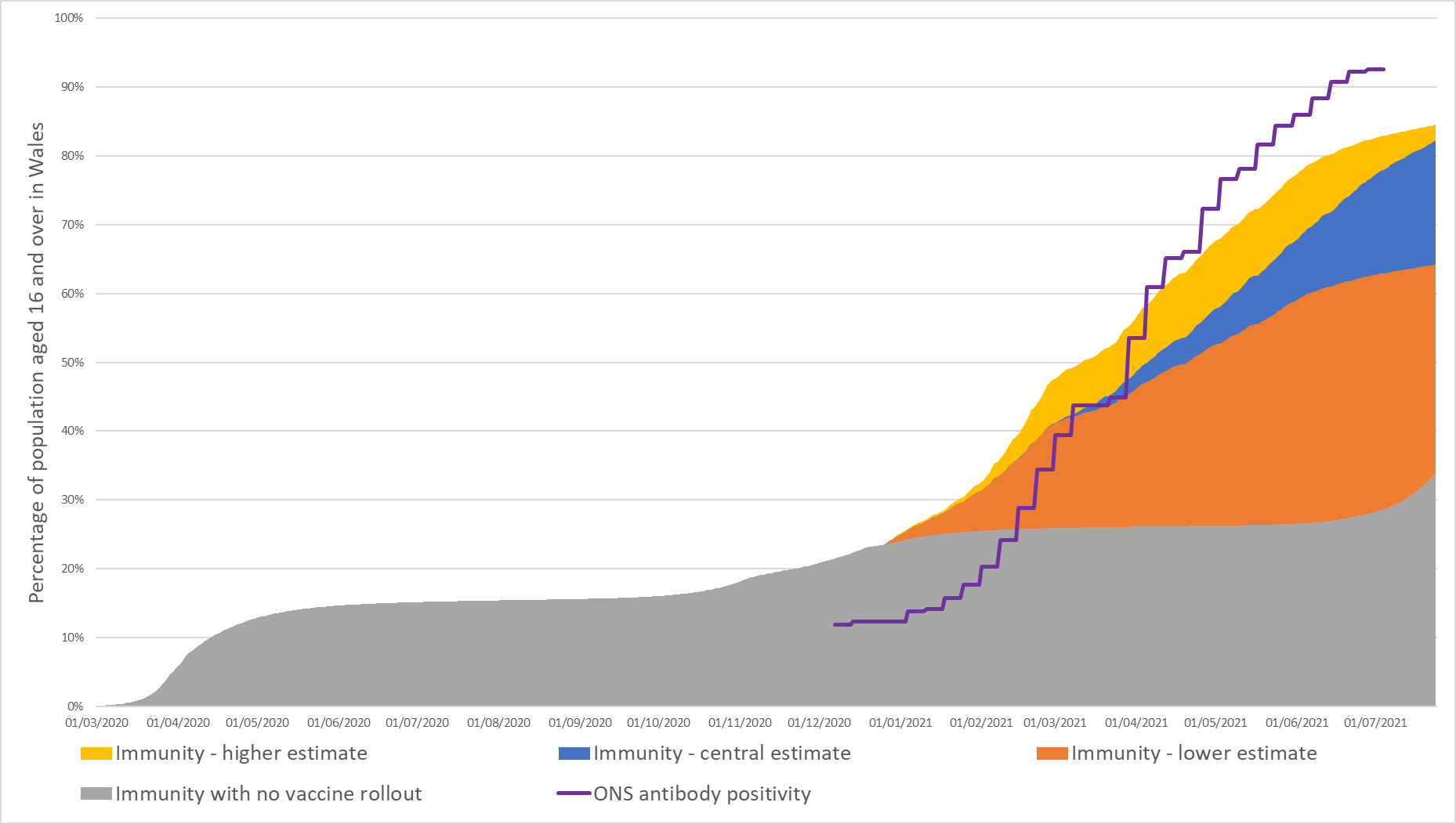
Figure 3 shows how the percentage of individuals aged 16 and over in Wales immune to COVID-19 infection has changed over time, assuming immunity wanes after 2 years. The vaccination programme clearly increased the growth of immunity level from January 2021. As more people become fully vaccinated, the central immunity estimate moves closer to the higher immunity estimate. Figure 3 also illustrates how the proportion immune to COVID-19 infection compares with and without the rollout of vaccines. At 24 July 2021, 82% of individuals aged 16 and over in Wales was estimated to be immune, compared with 34% had vaccines not been deployed.
Between 28 June and 4 July 2021, immunity was estimated to be between 76% and 78% of individuals aged 16 and over. This is lower than ONS’ estimate that 92.6% (91.0%, 94.0%) of the community population aged 16 and over had COVID-19 antibodies in the week beginning 28 June 2021. However, as discussed in Immunity compared with antibody positivity, antibody positivity is not equivalent to immunity.
Figure 4: Immunity estimates in Wales, by age group, to 24 July 2021, assuming immunity wanes after 2 years.

Figure 4 shows how immunity levels changed in different age groups over time. Sharp increases in immunity, particularly for the first priority groups reached, are observed when vaccine first doses became available to each priority group and when uptake of second doses increased. In contrast to older age groups, immunity estimates 12 to 15 year-olds remained fairly steady throughout 2021 because, at 10 July 2021, 12 to 15 year-olds were not routinely being offered a COVID-19 vaccine.
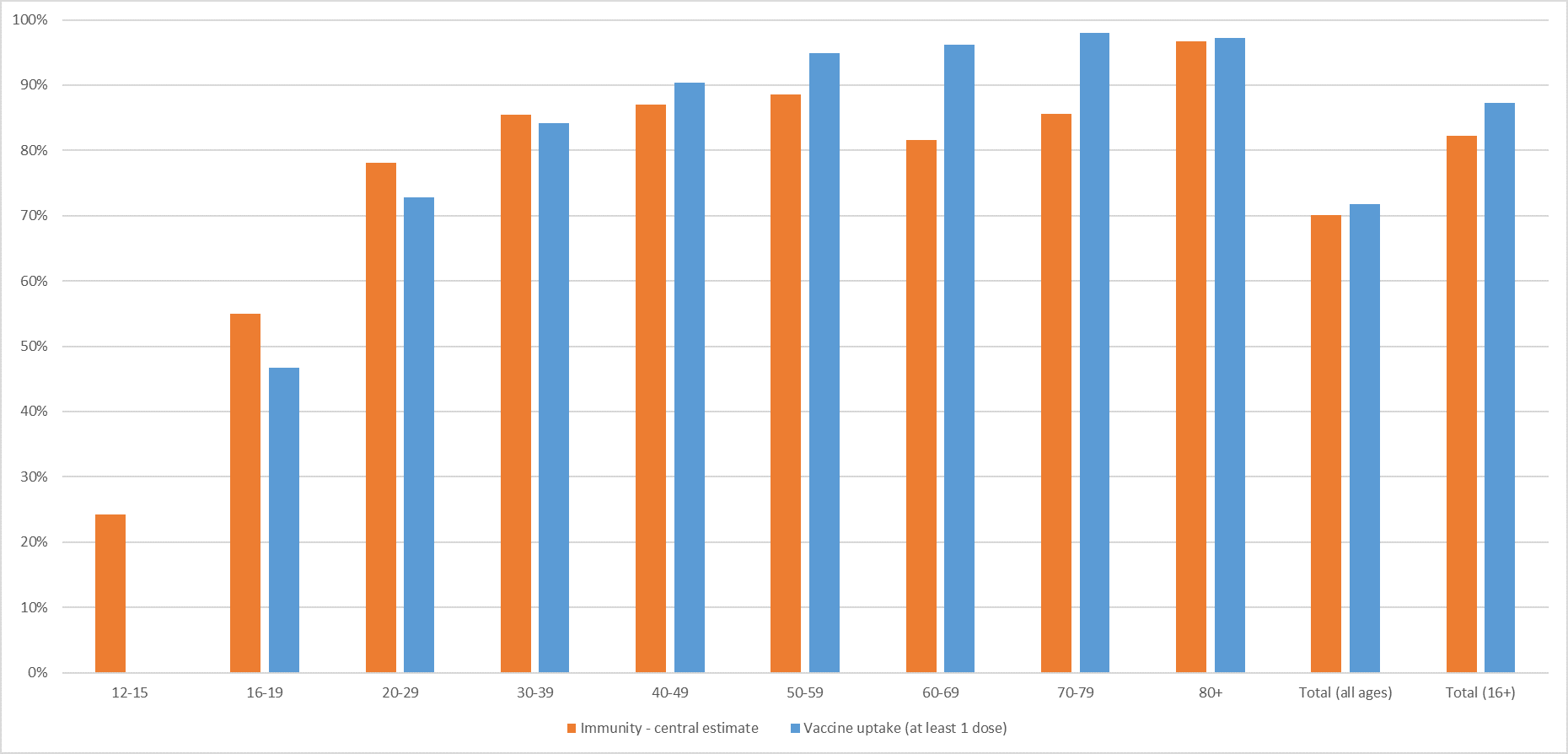
Figure 5: Immunity estimates and vaccine uptake in Wales, by age group, to 24 July 2021, assuming immunity wanes after 2 years.
Immunity estimates assuming immunity wanes after 10 months
Table 6 shows that 69% of individuals aged 16 and over in Wales and 58% of the total population in Wales were estimated to be immune to COVID-19 as at 24 July 2021. Without the introduction of COVID-19 vaccines, it was estimated that 18% of individuals aged 16 and over and 17% of the population would have been immune at 24 July 2021.
|
Age group |
Immunity [lower, upper] estimate |
Immunity estimate without vaccines |
|---|---|---|
|
16-19 |
39% [36%, 45%] |
20% |
|
20-29 |
59% [53%, 68%] |
24% |
|
30-39 |
68% [56%, 75%] |
23% |
|
40-49 |
73% [52%, 76%] |
19% |
|
50-59 |
76% [51%, 76%] |
17% |
|
60-69 |
73% [46%, 73%] |
11% |
|
70-79 |
78% [52%, 78%] |
9% |
|
80+ |
79% [51%, 79%] |
22% |
|
Total (all ages) |
58% [43%, 61%] |
17% |
|
Total (16+) |
69% [51%, 73%] |
18% |
Figure 6: Immunity estimates and antibody status of individuals aged 16 and over in Wales, to 24 July 2021, assuming immunity wanes after 10 months.
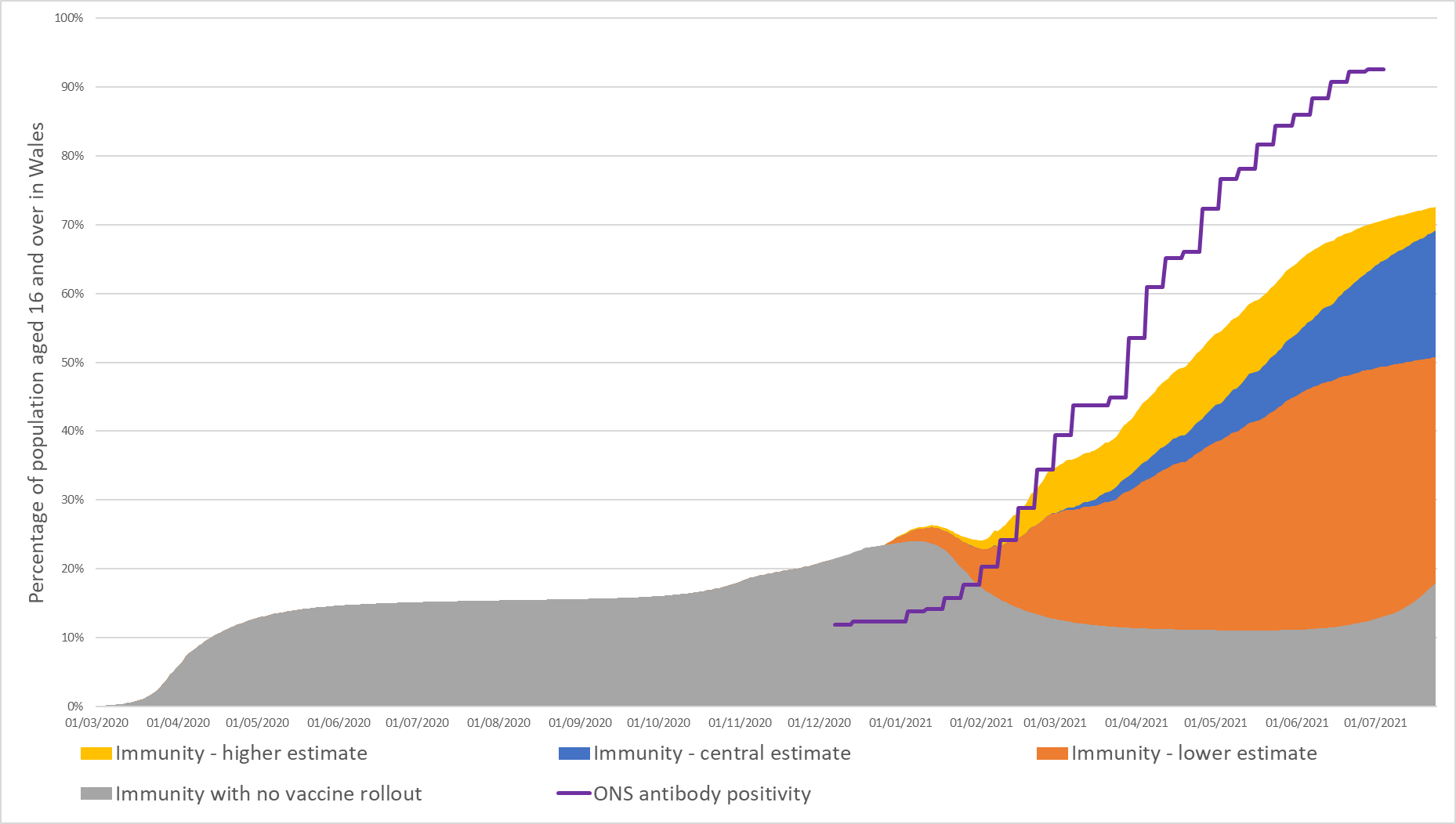
Figure 6 shows how the percentage of individuals aged 16 and over in Wales immune to COVID-19 infection has changed over time, assuming immunity wanes after 10 months. At 24 July 2021, 69% of individuals aged 16 and over in Wales were estimated to be immune, compared with 18% had vaccines not been deployed.
Figure 7: Immunity estimates in Wales by age group, to 24 July 2021, assuming immunity wanes after 10 months.
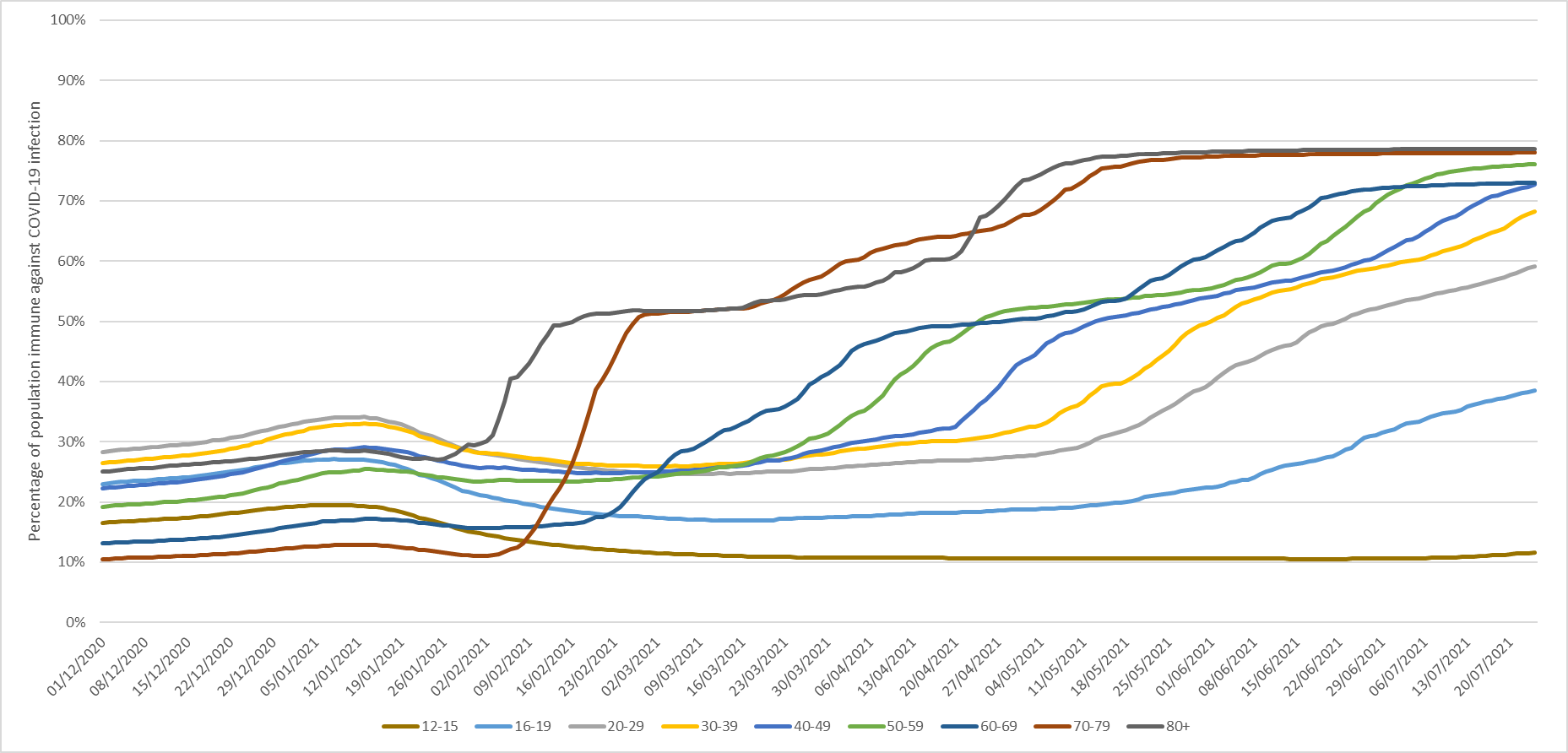
Figure 8: Immunity estimates and vaccine uptake in Wales by age group, to 24 July 2021, assuming immunity wanes after 10 month.

Immunity estimates assuming immunity wanes after 7 months
Table 7 shows that 63% of individuals aged 16 and over in Wales and 52% of the total population in Wales were estimated to be immune to COVID-19 as at 24 July 2021. Without the introduction of COVID-19 vaccines, it was estimated that 10% of individuals aged 16 and over and 10% of the population would have been immune at 24 July 2021.
|
Age group |
Immunity [lower, upper] estimate |
Immunity estimate without vaccines |
|---|---|---|
|
16-19 |
31% [28%, 38%] |
11% |
|
20-29 |
50% [44%, 59%] |
14% |
|
30-39 |
60% [47%, 67%] |
13% |
|
40-49 |
65% [45%, 69%] |
11% |
|
50-59 |
70% [44%, 71%] |
10% |
|
60-69 |
69% [42%, 69%] |
7% |
|
70-79 |
74% [49%, 75%] |
5% |
|
80+ |
71% [44%, 72%] |
12% |
|
Total (all ages) |
52% [37%, 55%] |
10% |
|
Total (16+) |
63% [44%, 67%] |
10% |
Figure 9: Immunity estimates and antibody status of individuals aged 16 and over in Wales, to 24 July 2021, assuming immunity wanes after 7 months.

Figure 9 shows how the percentage of individuals aged 16 and over in Wales immune to COVID-19 infection has changed over time, assuming immunity wanes after 7 months. In December 2020, immunity estimates agree closely with ONS’ antibody positivity. However, from March 2021, the antibody estimates grow at a faster rate than the immunity estimates.
The grey area shows that waning immunity greatly reduces immunity from natural infection alone. In this scenario, the growth in immunity level has started to slow in July 2021 because immunity started waning in individuals who were vaccinated in December 2020. Individuals vaccinated in winter 2020/2021 were the most clinically vulnerable, so loss of immunity in these groups is likely to lead to increased hospitalisations and deaths. This shows the importance of a booster vaccine programme around September 2021 to maintain immunity levels in the most vulnerable individuals and to reduce pressure on NHS resources and capacity. At 24 July 2021, 63% of individuals aged 16 and over in Wales were estimated to be immune, compared with 10% had vaccines not been deployed.
Figure 10: Immunity estimates in Wales, by age group, to 24 July 2021, assuming immunity wanes after 7 months.

Although immunity levels generally increased throughout 2021 due to the vaccine rollout, under this scenario, the increase was not uniform across the whole population. By July 2021, immunity started waning in individuals who were vaccinated in December 2020. In July 2021, this waning of immunity has the most impact on those aged 80 and over, who are among the most clinically vulnerable to COVID-19.
Figure 11: Immunity estimates and vaccine uptake in Wales by age group, to 24 July 2021, assuming immunity wanes after 7 months.

Discussion
For all scenarios, the vaccination rollout has significantly increased the level of immunity in the Welsh population. Generally, immunity estimates were higher for the older the age groups, as expected since vaccinations have been available longer for older age groups and a higher proportion of people in older age groups have hence been fully vaccinated.
Immunity estimates under the scenario where vaccines were not deployed to the population were generally higher for individuals aged 80 and over than for individuals aged 50-79. A driving factor for this could be that older individuals are more likely to require support in the home, more frequent hospital care, or be resident in care homes, which would increase the number of people they come into contact with and increase their risk of exposure to COVID-19. It could also because older age groups are more likely to be symptomatic and so get tested, therefore increasing the capturing of COVID-19 cases in older age groups compared with younger age groups.
Immunity estimates under the scenario where vaccines deployed were generally higher for individuals aged 16-49 than for individuals aged 50-79. A driving factor for this could be that younger individuals are more likely to have higher exposure to COVID-19 from increased social and work-based mixing.
Conclusion
Assuming immunity wanes after 2 years, 82% [64%, 85%] of people aged 16 and over in Wales and 70% [56%, 72%] of the total population in Wales were estimated to have had some immunity against COVID-19 infection at 24 July 2021.
Since it is estimated that over 80% (may be closer to 90%) of the Welsh population, spread evenly across Wales, must be immune to COVID-19 before population immunity effects could be observed, there is still a way to go before population immunity effects could be observed.
Glossary of terms
Susceptible population
The proportion of or number of people in Wales who do not have immunity to infection from COVID-19.
Immune population
The proportion of or number of people in Wales who have at least some immunity to COVID-19 disease due to vaccination or natural immunity following infection. The term “immune” used throughout this paper refers to individuals who are immune from being infected by COVID-19.
Efficacy
The proportion of people who, after 14 days following a COVID-19 vaccination dose, are considered to be immune to COVID-19 disease. For instance, for every 100 people given a 1st dose of a COVID-19 vaccine, after 14 days, 60 of those people are considered by the model to be immune to COVID-19 disease. Put another way, this means that 40 people are considered to still be susceptible to COVID-19 infection.
Antibody positivity
Antibody positivity is defined by a fixed amount of antibodies in the blood. A negative test result will occur if there are no antibodies or if antibody levels are too low to reach this threshold [footnote 12].
Footnotes
-
S1301_SPI-M-O_Summary_Roadmap_second_Step_4.2__1_.pdf (publishing.service.gov.uk)
-
S907_NERVTAG_certifying_COVID_immunity.pdf (publishing.service.gov.uk)
-
NERVTAG: Immunity certification update, 4 February 2021 - GOV.UK (www.gov.uk)
-
Vivaldi 2: COVID-19 reinfection in care homes study report - GOV.UK (www.gov.uk)
-
https://gov.wales/technical-advisory-cell-modelling-update-12-february-2021
-
Approximated using the average positive test count (UK Gov dashboard, cases by specimen date) / incidence in population (ONS CIS) ratio in England for the week to 28 March 2021 (data as at 10 May 2021). England data was used as the ONS COVID-19 infection survey does not estimate incidence for Wales due to low numbers.
-
Antibodies and Immunity – how do they relate to one another? | National Statistical (ons.gov.uk)