|
The goal: A society in which people’s physical and mental well-being is maximised and in which choices and behaviours that benefit future health are understood Author: John Morris, Welsh Government What have we learnt from the data in the last year?Most headline measures for health show little or no change over the most recent year, such as life expectancy, percentage of babies born with a low birth weight and the percentage of people with fewer than two positive lifestyle behaviours. Recent data do show that after years of sustained increases, gains in life expectancy have continued to slow and even stop. This is true across the UK and is also evident elsewhere globally. However, increases in life expectancy in the UK were small compared to a number of other countries. There was no significant change in any of the 5 main healthy lifestyle behaviours (not smoking, not drinking over weekly guidelines, fruit and vegetable consumption, physical activity, healthy weight) between 2016-17 and 2017-18. The picture for child health continues to be mixed, for example there have been improvements in dental health, but child obesity increased over the year and is similar to four years ago. Measuring well-being is complex and well-being changes throughout your life course. Analysis shows that during secondary school there are some dramatic changes in children’s well-being, self-reported health and lifestyles. Whilst at age 11 girls and boys report similar well-being and self-reported health, by aged 16 a gap is evident, with girls reporting lower well-being and worse health. Mental well-being improves from younger ages until very old ages but life satisfaction dips during middle age. Girls score significantly poorer than boys on the moods and feelings scale and are more likely to self harm. Self-reported very bad or bad health was the strongest factor associated with the poorest personal well-being for adults. Health was also the most important factor when looking at mental well-being. For most types of cancer, survival decreases as stage at diagnosis becomes
later - the gradient of the decrease from earlier to later stages varies
considerably between different cancer types. Whilst survival rates in Wales
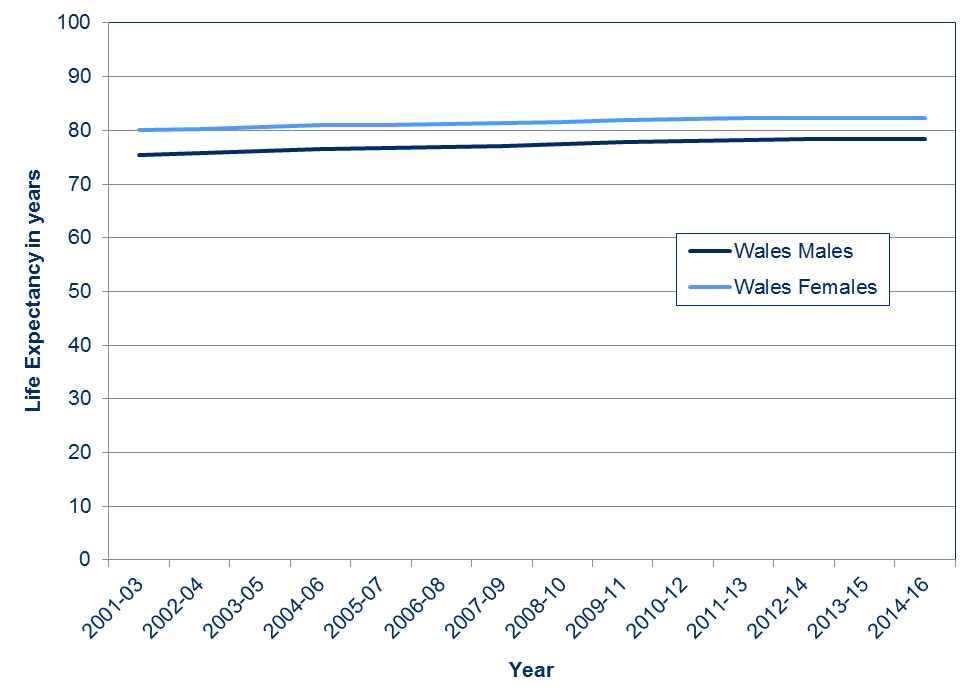
compare poorly to Europe, they are similar to England. After years of sustained increases, improvements in life expectancy have stalledLife expectancy has risen by 3.0 years for men and 2.2 years for women since the period 2001 to 2003, with the gap between male and female life expectancy closing. A girl born in Wales between 2014 and 2016 could expect to live to her 82nd birthday while a boy could expect to reach his 78th. However, the last three or four years have seen no increase in life expectancy. Research by the Office for National Statistics shows that this is true for both England and Wales and that the slowdown in mortality improvements over the last decade affects all ages. Further reports show this slowdown was seen across all four UK countries (though with a greater slowdown in England & Wales). It was also evident in many other countries internationally, though the UK experienced one of the largest slowdowns. The report also noted that Japan has come through a period with low life expectancy gains and has recently experienced an acceleration of mortality improvements, showing that even after a period of slow growth a country may again return to faster improvements. 3.01 Life expectancy at birth by sex, 2001-03 to 2014-16
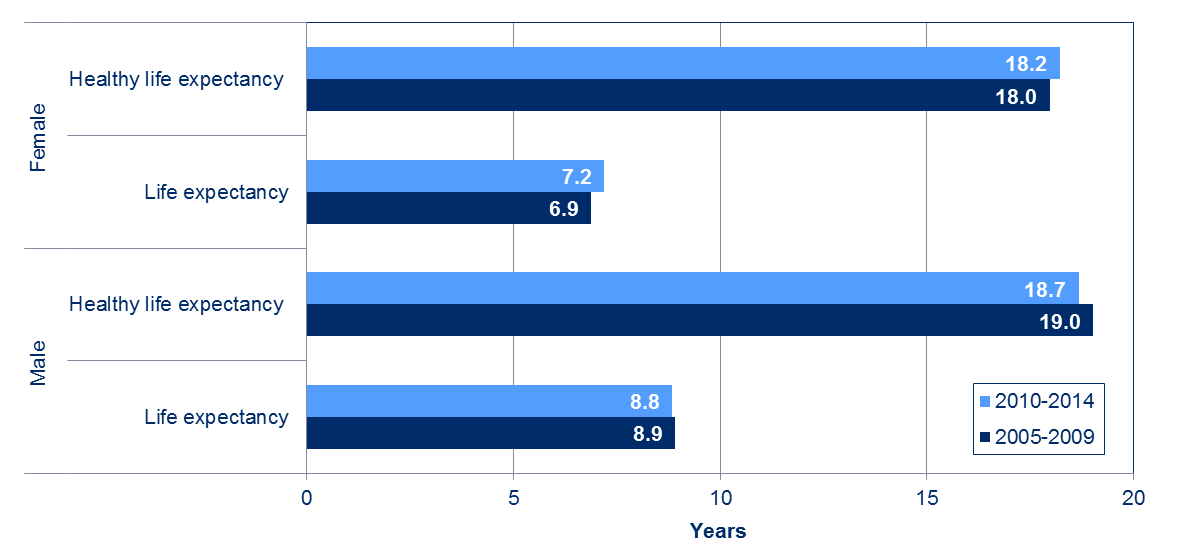
Healthy life expectancy remains unequal across WalesDeprivation is strongly linked to life expectancy – people born into deprived families will have shorter healthy life expectancy. This is reflected in the healthy life expectancy gap between the most and least deprived areas of Wales and this hasn’t changed in the most recent years. 3.02 Gap in life expectancy between the most and least deprived parts of Wales, 2005 to 2014
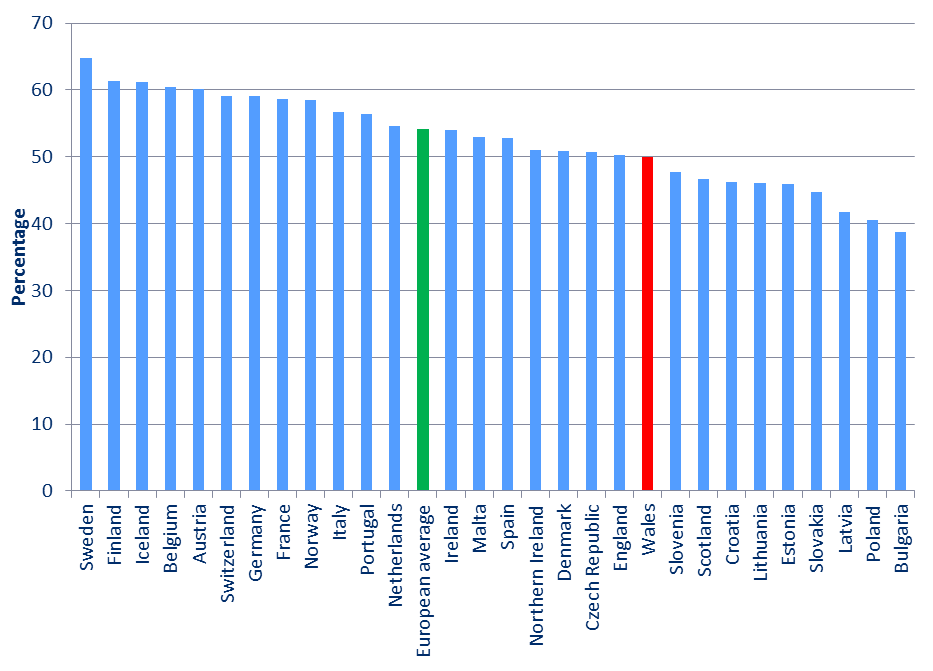
Source: Public Health Wales Observatory More recent analysis by the Office for National Statistics shows that the gap between the most and least deprived (using deprivation deciles rather than quintiles) remained broadly similar over recent years. Self-reported general health changes in secondary school more for girls than boys and deteriorates significantly in later lifeHow long do you expect to live in good health? Well, the length of time a person in Wales can expect to live in good health was increasing (based on those who self reported that their health is good). However as with life expectancy it has stalled with little change over the last five years. Because girls live longer, the percentage of their life expected to be spent in good health is lower than for boys: 76 per cent of a girl’s life and 79 per cent of a boy’s life. From year 9 onwards more girls report fair/ poor health than boys. At age 11 (year 7) the proportion of boys and girls reporting poor health is the same (one in seven), but by age 16 (year 11) there is a gap – with one in three girls reporting poor health compared to one in four boys. However the overall proportion of children reporting poor health has fallen – down from 26 per cent in 2002 to 22 per cent in 2018. That fall is most evident in girls, but year 11 girls have seen little change over the last 12 years. Adults self-reported general health in Wales has been improving over time for older adults, but has deteriorated slightly for younger adults (driven by more younger adults reporting being treated for mental health conditions). Self-reported health does deteriorate with age, with 83 per cent of 16-24 year olds reporting good or very good health compared to 49 per cent of those aged 75 or over. Cancer survival in Wales is in line with England and new analysis shows early diagnosis is importantThere are no significant differences in five year survival between Wales and England for any of the cancer types, and the same is true for nearly all cancer types for one year survival. However, survival rates are shown to be lower in Wales than most other European countries (based on Eurocare 5, 2000-2007, with 5 year survival (i.e those surviving for 5 years after diagnosis of cancer) around 4 percentage points less than the European average for all cancer types. 3.03 5 year cancer survival rates (2000-2007, relative, age-standardised)
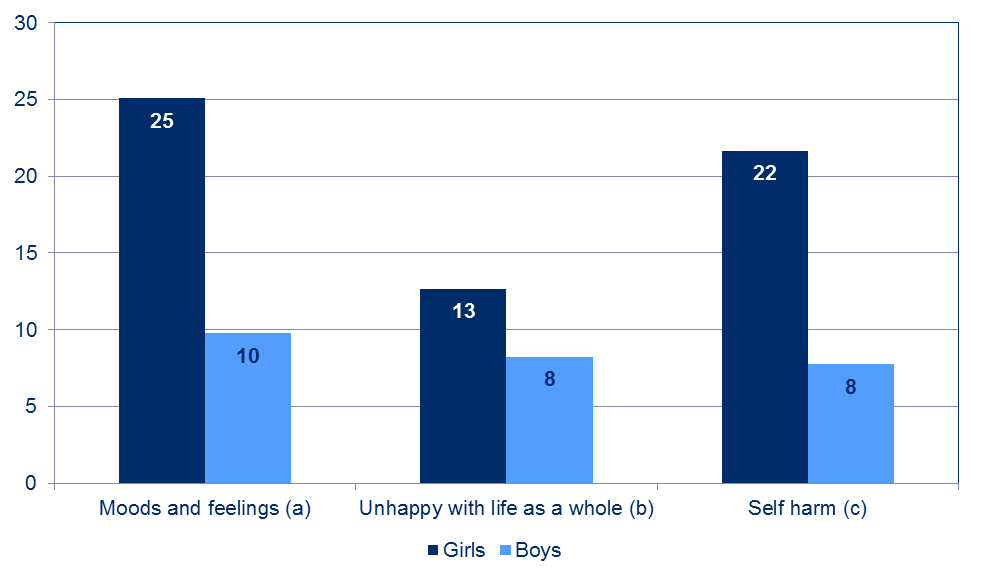
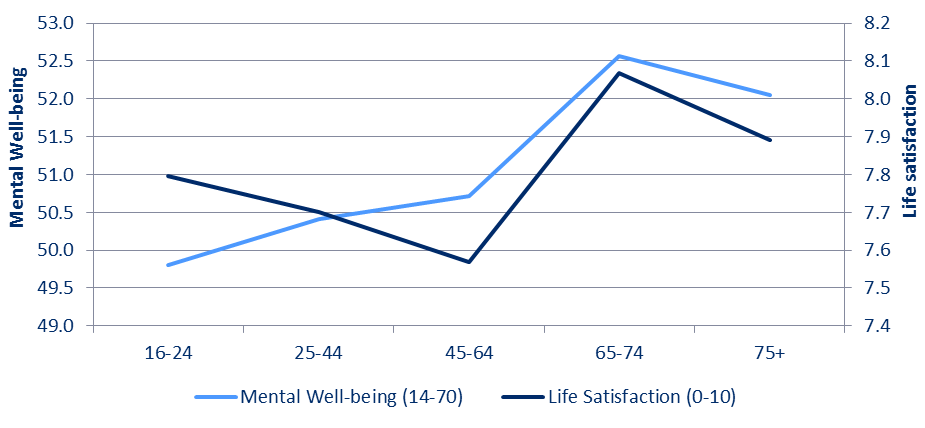
Source: Eurocare 5 For most types of cancer, survival decreases as stage at diagnosis becomes later - the gradient of the decrease from earlier to later stages varies considerably between different cancer types. Men have better survival than women in later or unknown stages at diagnosis for many cancers, except for lung cancer and melanoma. Your well-being changes during your life – it deteriorates whilst you are in secondary school (especially for girls) then improves in older agesSelf-rated life satisfaction decreases for girls from year 7 (aged 11) through to year 11 (aged 16) and is notably lower than boys. Overall, self-rated life satisfaction has remained at a similar level during the last decade or so, from 2002 to 2018. Life satisfaction for adults shows small increases over time and it is generally similar to other UK nations. However, in the year ending December 2017, a larger proportion of people in Wales reported low levels of life satisfaction, worthwhile and happiness compared to the UK average. For example, 4.3 per cent of people in Wales reported a score of 0 to 4 for their worthwhile ratings compared with only 3.4 per cent in the whole of the UK. However, there was no significant difference in anxiety ratings between Wales and the UK average. 3.04 Mental well-being results for boys and girls aged 14, 2015, Wales
(a) Percentage with high score (12 or more out of 26) on Moods & Feelings scale (b) Percentage with low score (below mid-point) for happiness with life as a whole (c) Percentage who have hurt themselves on purpose in any way in the past year Source: Millennium Cohort Study
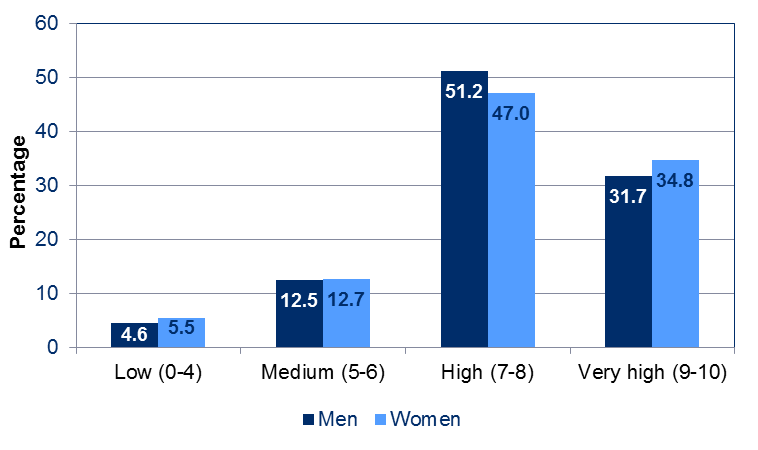
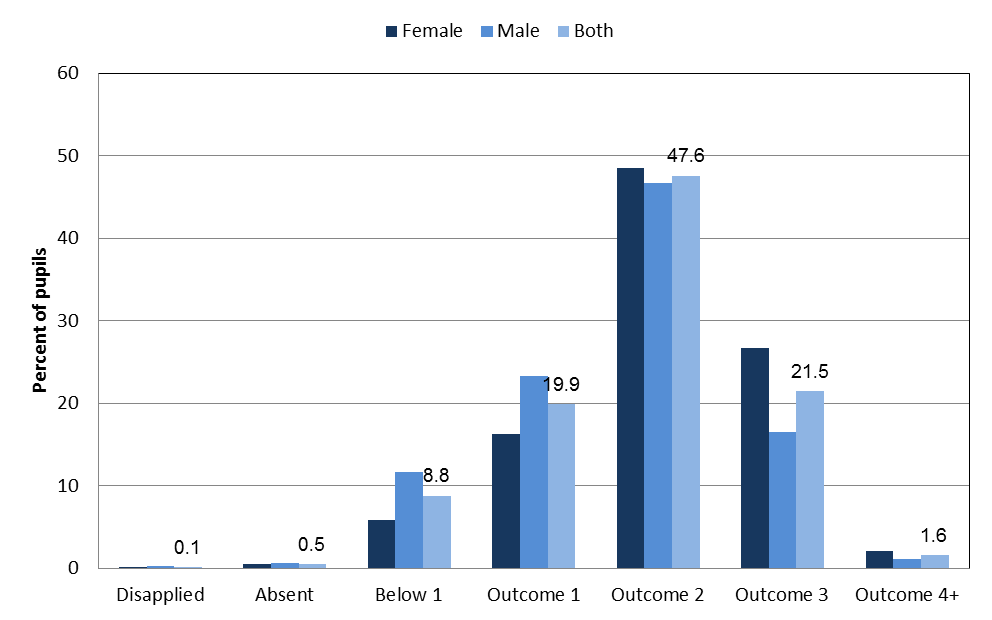
Girls score significantly poorer than boys on the moods and feelings scale and a higher proportion of them have self-harmed in the previous year. Analysis of data from the School Health Research Network shows that mental well-being is broadly the same for boys and girls at year 7 but by year 10 girls’ mental well-being has fallen more so than for boys. A higher percentage of boys than girls (19 per cent vs 13 per cent) reported bullying another child in 2018, but this has fallen during the last decade. However, a greater percentage of girls reported being bullied than boys (38 per cent vs 33 per cent), with evidence that this has increased in the most recent years to 2018. Overall for secondary school pupils 35 per cent had been bullied in the previous two months while 9 per cent had been bullied at least once a week. 3.05 Life satisfaction and mental well-being by age, 2016-17 Source: National Survey for Wales Whilst mental well-being continues to improve until very old ages, life satisfaction dips during middle age. The chart above shows that although young adults (16-24) have the lowest average mental well-being scores, they have higher life satisfaction scores than those aged 25-64. Average mental well-being scores for women are consistently lower than men across all age groups. Although life satisfaction scores are a little higher for women than men on average (7.8 vs 7.7), more women report having very low life satisfaction scores and very high life satisfaction scores as shown in the chart below. In 2017-18, around 9 per cent of adults reported a long-standing mental disorder. 3.06 Life satisfaction by gender, 2017-18 A range of other factors are also important to physical and mental well-being, and many of these are included in the public health outcomes framework. When controlling for a range of factors, better mental well-being was found to be associated most strongly with being in good health. Not being in material deprivation and being older were also shown to be among the most important factors in good mental well-being for adults. A range of factors influence well-being. A report from the Office for National Statistics states that health was the main factor for personal well-being, followed by work situation and relationship status. In terms of employment, data show a big improvement in the employment rate in Wales over the period since devolution, with an employment rate of 74.8 per cent for the period May to July 2018, 0.7 per cent below the UK figure. However the gap in the employment rate for those aged 16 and over between those with a long term health condition and those who do not have one persists, and was 15.9 percentage points in 2017. The suicide rate for those people who are divorced is more than twice as high as those who are single, whilst those who are in a relationship have the lowest rate. Where you live is important to well-being (and health as well) with access to green space and community cohesion affecting how people feel. In general air quality in Wales has greatly improved since the 1970s, due mainly to statutory emissions controls and a decline in heavy industry. However, pollution from other sources, such as transport, agriculture and domestic heating has become more of a concern. The highest concentrations of nitrogen dioxide emissions are found in large urban areas and adjacent to busy roads. Public Health Wales estimates that the equivalent of around 1,600 deaths are attributed to PM2.5 exposure, and around 1,100 deaths to NO2 exposure, each year in Wales (as there are overlapping health impacts of individual pollutants, it is not possible to sum these). Those in good health report much higher (positive) mental well-being scores (using the Warwick-Edinburgh Mental Well-Being Scale) than those who are not in good health. Adverse experiences in childhood have long lasting effects, but sports participation at a young age can help resilience in later lifeResults from the first Welsh Adverse Childhood Experience (ACE) study show that when comparing people who suffered four or more harmful experiences in childhood with those who suffered none, those who suffered were 4 times more likely to experience high-risk drinking in adulthood, 6 times more likely to be a smoker and 14 times more likely to be involved in violence in the last year. The second survey showed a similar pattern and that those people who have suffered four or more ACEs were 6.1 times more likely to have ever been treated for a mental illness. Having some resilience resources more than halved risks of current mental illness in those with four or more ACEs. The ACEs report also showed that there are strong relationships between sports participation in childhood and lower lifetime mental illness. There are also associations between regular adult participation in sports and current mental illness. The National Survey for Wales showed that, in 2017-18, 59 per cent of people had participated in some sport or physical activity in the past 4 weeks. By far the most commonly-reported activity was to have walked more than 2 miles (33 per cent of people), followed by attending the gym or fitness classes (16 per cent), indoor swimming (13 per cent) and jogging (11 per cent). 11 per cent of adults participated in a sporting or physical activity around once a week, 8 per cent participated twice a week, and 32 per cent at least three times a week. Women were less likely to participate in sport, with 45 per cent having no frequent activity compared to 35 per cent for men. A child’s early years are a key time to help to ensure good outcomes later in lifeThe number of single babies (as opposed to twins or triplets etc.) born weighing less than 2.5 kg (5 pounds, 8 ounces) has been falling over the last decade or so. The most recent statistics for 2017 showed that 5.6 per cent of births (single babies) were low birth weight in Wales. This is the highest percentage since 2009. A range of factors can result in low birth weight, for example smoking in pregnancy, anaemia, substance misuse and poor sexual health. The rate for all live births in Wales was 6.8 per cent in 2015 (this includes non singleton births) which was slightly above that of the OECD average (6.5 per cent). But while the OECD average increased 0.4 percentage points between 2001 to 2015, the rate for Wales has fallen. Low birth weights are strongly linked to deprivation. The most recent analysis, using data from 2012 to 2014, showed that the most deprived fifth were 30 per cent more likely to have a single baby with a low birth weight than the middle fifth. Breastfeeding has health benefits for babies and their mothers. The percentage of babies breastfed at birth has risen from 55 per cent in 2006 to 61 per cent in 2017. Babies of older mothers are more likely to be breastfed than those of younger mothers. Breastfeeding rates have increased, although only around 60 per cent of mothers who began breastfeeding at birth are still doing so at 6-8 weeks. The most recent figures on children’s dental health (aged five and twelve) both show an improvement. There has been a reduction in the proportion of children aged five with decay over the last decade or so and although the proportion of children with dental decay is higher in the most deprived areas than the least, that gap is narrowing. For those aged twelve there have been continued reductions in the prevalence of dental caries across all deprivation quintiles between 2004 and 2017. Despite this, the ratios of dental caries for the most deprived versus the middle deprived groups appear to be widening albeit slightly. Teenage conceptions reached a record low in Wales in 2016 and have fallen dramatically since 2008. The rate for those aged under 18 has more than halved over the same time period. New data are available on children’s stages of development on entry into primary schoolChildren in Wales are assessed through the Foundation Phase Profile, during their first 6 weeks following entry into primary school (Reception Class). This is used to determine the stage of development and interests of the child according to the according to the Foundation Phase Profile and framework. The data reflect the wide range of developmental maturity that we expect at this age, which is well within the normal range for children at entry to school, especially with the age variability at the point of school entry. One of the areas in which children are assessed is in personal and social development, well-being and cultural diversity. Around 7 in 10 pupils aged 4 are at a stage of development in this area of learning that would be consistent with, or greater than their age according to the framework, with around 9 in 10 pupils within one stage of the development consistent with their age. 3.07 On-entry assessments of pupils in reception class: personal and social
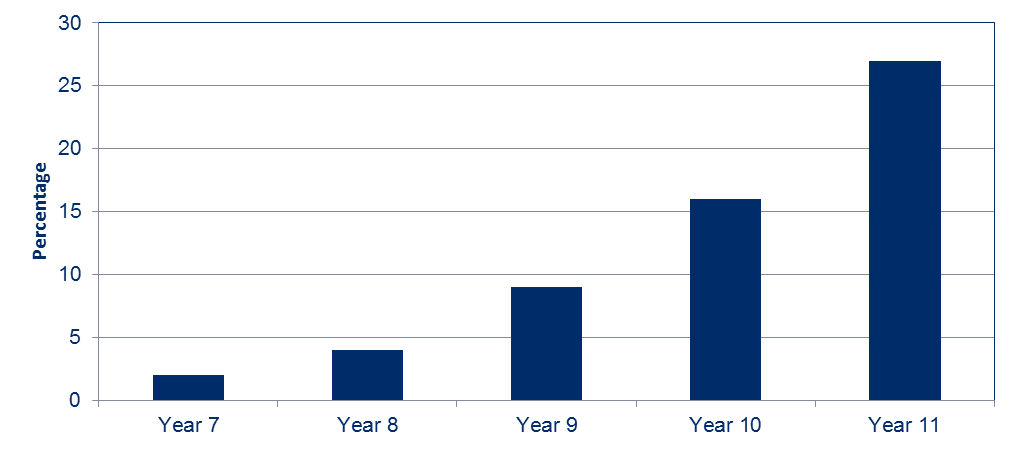
development Source: On-entry assessments of pupils, Welsh Government Most health behaviours begin to deteriorate in secondary school, but improve in older age10 per cent of those aged 16 or over and 12 per cent of 11 to 16 year olds showed fewer than two healthy lifestyle behaviours (not smoking, not drinking above guidelines, consuming five fruit and veg a day, meeting physical activity guidelines and (for adults) healthy weight). For children, the number of healthy lifestyle behaviours deteriorates with age. 2 per cent of pupils in year 7 had fewer than two healthy lifestyle behaviours, increasing to 9 per cent in year 9 and 27 per cent in year 11. 3.08 Percentage of children following fewer than two healthy lifestyle behaviours by school year, 2013/14
Source: Health Behaviour in School aged Children (HBSC) Boys are more likely to be obese or overweight in school, with the gap widening during secondary school and until middle age, when it starts to reduce again. 3.09 Percentage of children aged 11-16 following selected health behaviours
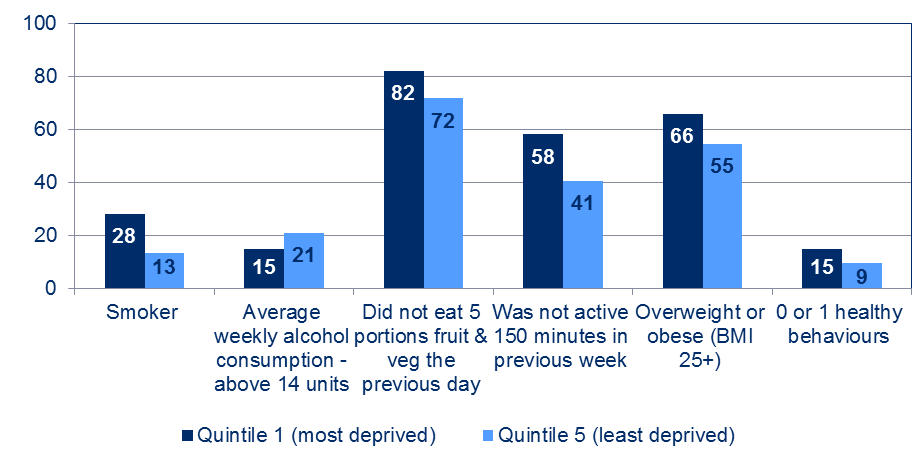
Source: Health Behaviour in School-aged Children and School Health Research Network Rates of smoking have declined since 1998 for 11 to 16 years olds from 13 per cent to around 4 per cent in 2017/18. Rates of drinking among young people on a weekly basis have fallen significantly between 2002 (23 per cent) and 2017/18 (9 per cent). Participation in physical activity is little changed from 2002 with boys being consistently more likely than girls to be physically active. Data for 2017/08 is provisional. Around a third of secondary school children walk to school, with a slightly higher proportion of boys than girls walking to school. Smoking rates and the percentage of people consuming excess alcohol in Wales have both gone down over time. But while there are some positive trends, challenges remain and the more deprived areas of Wales face greater challenges. 15 per cent of adults in these areas show fewer than two healthy lifestyle behaviours compared with only 9 per cent in the least deprived areas. Whilst almost all of the lifestyle behaviours were ‘worse’ in the most deprived areas, adults were less likely to drink above weekly alcohol guidelines in the most deprived areas than the least deprived areas. 3.10 Adult lifestyles by deprivation quintile, 2017-18 Source: National Survey for Wales Those who are in material deprivation are more likely to struggle to afford a healthy diet. 2 per cent said they cannot afford to eat meals with meat, fish (or a vegetarian equivalent) at least every other day whilst 4 per cent said that there had been at least one day in the previous fortnight where they had needed to go without a substantial meal due to lack of money. Older people were less likely to be in material deprivation than young or middle-aged people. |